Tennis Elbow Recovery Time Estimator
Estimate Your Recovery Timeline
Based on severity, treatment approach, and adherence to your home management plan
Tip: Consistent adherence to your home exercise program significantly improves recovery outcomes.
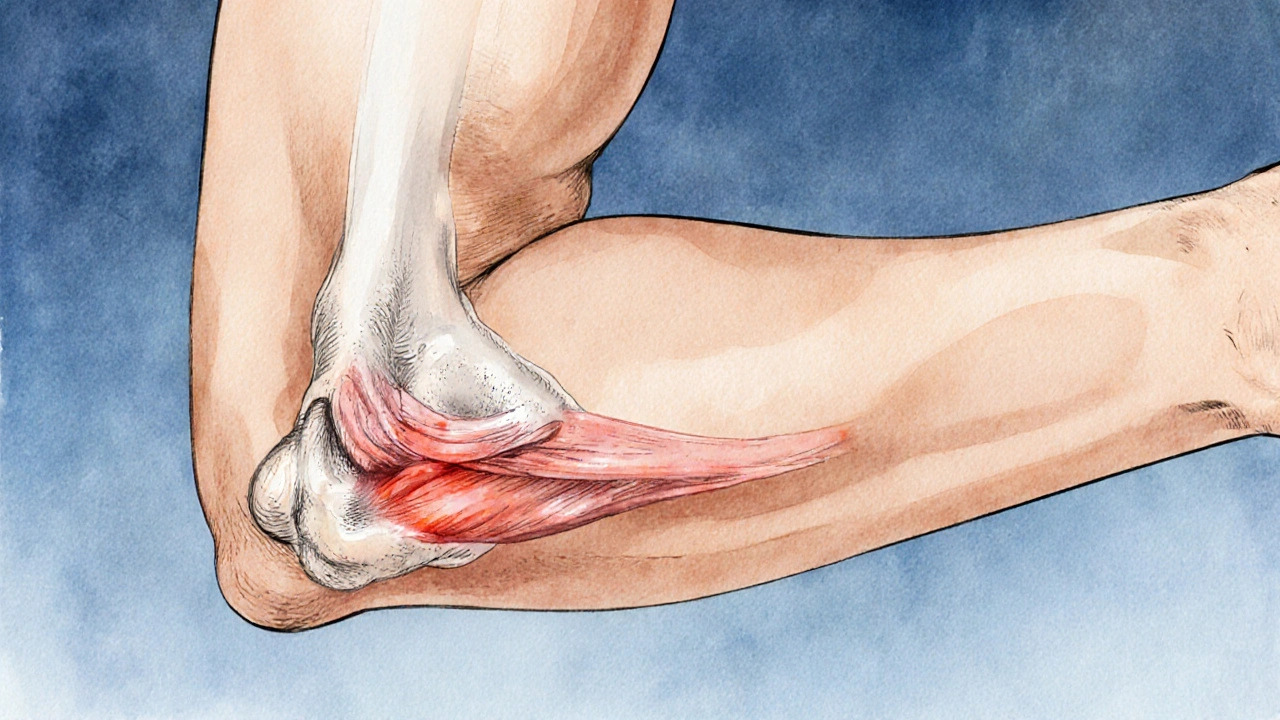
Lateral Epicondylitis is a common overuse injury that affects the outer part of the elbow. It’s the medical name for what most people call tennis elbow. The condition occurs when the common extensor tendon, which attaches to the lateral epicondyle of the humerus, becomes inflamed or micro‑torn due to repetitive strain.
What Triggers Lateral Epicondylitis?
Even though the name suggests a tennis‑related problem, the injury shows up in anyone who repeats wrist‑extension or forearm‑pronation motions. Typical triggers include:
- Racket sports - especially backhand strokes that force the forearm muscles to contract forcefully.
- Manual labour - painters, carpenters, and plumbers often lift tools that strain the elbow.
- Computer use - prolonged mouse clicking or typing with a tight grip can accumulate micro‑damage.
- Bad equipment - grip size that’s too small or too large forces the forearm muscles to work harder.
When the load exceeds the tendon’s capacity to repair, tiny tears appear. The body’s inflammatory response then causes pain, swelling, and reduced grip strength.
Spotting the Symptoms
Even a mild case can hamper daily activities. Look out for these signs:
- Sharp or aching pain on the outer elbow, especially when gripping or lifting.
- Stiffness that worsens after periods of inactivity (like waking up in the morning).
- Weakness when trying to turn a screwdriver or shake hands.
- Pain that radiates down the forearm toward the wrist.
If you notice any of these, an early visit to a physiotherapist or primary‑care doctor can prevent chronic problems.
Key Anatomy: The Extensor Carpi Radialis Brevis (ECRB)
Extensor carpi radialis brevis (ECRB) is the muscle most often blamed for lateral epicondylitis. It originates near the elbow and extends the wrist. Because the ECRB shares its tendon with the common extensor group, it bears a disproportionate share of the repetitive load.
When the ECRB’s tendon is overworked, microscopic degeneration - called tendinosis - sets in. This is why “tennis elbow” is technically a tendonitis/tendinosis condition rather than a simple inflammation.
Diagnosing the Condition
Doctors usually start with a physical exam. They’ll ask you to perform a series of maneuvers, such as:
- Resisted wrist extension - the doctor presses against your hand while you try to lift your wrist.
- Cozen’s test - you make a fist, extend the wrist, and the doctor palpates the lateral epicondyle.
If the exam is inconclusive, imaging may be ordered:
- Ultrasound - shows tendon thickening or tears in real‑time.
- MRI - provides a detailed view of soft‑tissue damage.
Most cases are identified clinically; advanced imaging is reserved for persistent or atypical symptoms.

Non‑Surgical Treatment Options
For 80‑90 % of patients, conservative care resolves the problem in 3‑6 months. Below is a quick rundown of the most common approaches.
| Treatment | How It Works | Typical Course | Evidence of Effectiveness |
|---|---|---|---|
| Physiotherapy | Progressive loading, stretching, and manual therapy to remodel tendon fibers. | 2‑3 sessions per week for 6‑8 weeks. | Systematic reviews show 70‑80 % success when protocols include eccentric loading. |
| Corticosteroid Injection | Anti‑inflammatory medication injected around the tendon. | Single injection; may repeat after 4‑6 weeks. | Provides rapid pain relief but high relapse rate after 3 months. |
| Shockwave Therapy | High‑energy acoustic waves stimulate neovascularization. | 3‑5 sessions spaced a week apart. | Meta‑analysis reports ~60 % patients experience meaningful improvement. |
| Platelet‑Rich Plasma (PRP) | Autologous concentration of platelets injected to promote healing. | 1‑2 injections, 4 weeks apart. | Emerging evidence; 55‑65 % success in randomized trials. |
| Rest & Activity Modification | Reducing aggravating movements and using ergonomic tools. | Variable; often combined with other therapies. | Fundamental; alone rarely resolves moderate‑to‑severe cases. |
| Bracing (Counterforce Strap) | Compresses forearm muscles to off‑load tendon. | Worn during activity for 2‑4 weeks. | Provides modest pain reduction; best as adjunct. |
Most clinicians start with physiotherapy and activity modification, reserving injections or shockwave for stubborn pain.
Step‑by‑Step Home Management Plan
- Identify the aggravating activity. Keep a simple log of when pain spikes - e.g., after 30 minutes of racquet play.
- Apply ice for 10‑15 minutes, three times a day, during the first 48 hours of flare‑up.
- Start gentle wrist extensor stretches: straighten the arm, palm down, pull the hand toward you with the other hand for 20‑30 seconds, repeat 3×.
- Progress to eccentric loading: hold a light dumbbell (1‑2 kg), lower the wrist slowly over 3 seconds, then use the opposite hand to return to start. Perform 2 sets of 15 reps twice daily.
- Consider a counterforce strap during activities. Place it 2‑3 cm distal to the lateral epicondyle and tighten until you feel comfortable pressure.
- Schedule a physiotherapy session within a week to fine‑tune the program and add manual mobilizations.
Consistency is key. Most patients notice a drop in pain after 2‑3 weeks if they stick to the plan.
When to Seek Professional Help
While many cases resolve with self‑care, watch for red flags that merit a clinician’s eyes:
- Pain that persists beyond 12 weeks despite home measures.
- Significant loss of grip strength (more than 30 % compared to the other side).
- Numbness or tingling down the forearm - may indicate nerve involvement.
- Visible swelling, bruising, or a palpable lump near the elbow.
Early intervention can prevent chronic tendinosis that sometimes requires surgical release.

Surgical Options - A Last Resort
If conservative care fails after 6‑9 months, orthopedic surgeons may discuss two main procedures:
- Open or arthroscopic release of the common extensor tendon - cuts the damaged tissue to allow healthy regrowth.
- Debridement plus repair of the ECRB origin - removes scar tissue and re‑anchors the tendon.
Success rates hover around 85 % with a typical rehab timeline of 3‑4 months before returning to full activity.
Prevention: Protect Your Elbows for Life
Even if you never pick up a racket again, the same mechanics can crop up in everyday tasks. Here are easy habits to keep the tendons happy:
- Warm up with arm circles and light wrist stretches before any repetitive work.
- Use tools with ergonomic handles; switch hands when possible.
- Strengthen forearm extensors with dumbbell curls and reverse curls twice weekly.
- Take micro‑breaks - a 30‑second pause every 15 minutes reduces cumulative loading.
Prevention is cheaper, faster, and less painful than treating a flare‑up.
Frequently Asked Questions
Is tennis elbow only a problem for tennis players?
No. The condition is an overuse injury of the forearm extensors, so anyone who repeatedly lifts, grips, or twists can develop it - from carpenters to office workers.
Can I treat tennis elbow without a doctor?
Mild cases often respond to home exercises, ice, and activity modification. If pain lasts more than a few weeks or worsens, a professional evaluation is advisable.
How long does recovery usually take?
Most people feel significant improvement within 6‑8 weeks of a structured physiotherapy program. Full recovery can take up to 4‑6 months for severe cases.
Are corticosteroid injections safe?
They are safe when administered by a qualified clinician, but they can weaken tendon tissue if used repeatedly. Most doctors limit injections to one or two rounds.
What’s the difference between shockwave therapy and PRP?
Shockwave uses acoustic energy to stimulate healing, while PRP injects a concentrated mix of your own platelets to release growth factors. Both aim to kick‑start tendon repair, but the evidence for PRP is newer and varies by clinic.





Alex Lineses October 18, 2025
Great overview of lateral epicondylitis! The description of eccentric loading and progressive tendon remodeling captures the essential physiotherapy principles. If you're dealing with a grip‑strength deficit, incorporating a handheld dynamometer can quantify baseline force and track improvements over the 6‑8 week protocol. Also, consider adjusting the counterforce strap placement slightly distal to the epicondyle to optimize load distribution. Remember, consistent micro‑breaks and ergonomic tool handles synergize with the loading program to prevent recurrence.
Brian Van Horne October 18, 2025
In summation, the elucidation herein is both perspicacious and mellifluous.
Norman Adams October 18, 2025
Ah, another masterclass in elbow biomechanics-because clearly, everyone has been waiting all their lives to learn about the extensor carpi radialis brevis while sipping lattes.
Margaret pope October 18, 2025
Thanks for the solid tips your info really helps anyone dealing with a sore elbow try the eccentric loading and keep a log of pain spikes you’ll see progress faster
Karla Johnson October 18, 2025
When I first encountered tennis elbow as a carpenter, I was surprised at how quickly the discomfort escalated from a mild ache after a day of framing to a debilitating pain that prevented me from even holding a hammer. The article correctly identifies repetitive wrist extension as the primary antagonist, yet many patients overlook the subtler contribution of forearm pronation during tool manipulation. In my experience, a comprehensive assessment should begin with a functional movement screen that isolates the ECRB while monitoring scapular stability, because upstream deficits often masquerade as local tendon pathology. Once the baseline is established, I prescribe a graduated eccentric protocol using a lightweight dumbbell, emphasizing controlled descent over three seconds and a brief pause before concentric assistance. Concurrently, I integrate proprioceptive neuromuscular facilitation (PNF) stretching to enhance sarcomere length and reduce passive tension. Nutrition also plays a non‑trivial role; adequate collagen synthesis requires vitamin C and hydrolyzed gelatin supplementation, especially during the reparative phase. Moreover, ergonomic modifications-such as swapping to a pistol grip drill with a larger handle-can drastically reduce the cumulative load on the extensor tendons. It is essential to educate patients about micro‑breaks: a thirty‑second pause every fifteen minutes of repetitive activity has been shown to attenuate inflammatory markers. For those who persist despite conservative measures, I recommend a diagnostic ultrasound to differentiate tendinosis from focal partial tears, guiding the decision to consider PRP versus continued load management. While corticosteroid injections provide rapid analgesia, they may impair collagen remodeling if overused, so I reserve them for acute flare‑ups only. Shockwave therapy, though promising in the literature, should be adjunctive and not a first‑line treatment. Finally, documenting progress through objective grip dynamometry every two weeks helps maintain motivation and allows timely adjustments to the program. In summary, a multimodal approach that blends biomechanical correction, progressive loading, nutritional support, and patient education yields the most reliable resolution of lateral epicondylitis.
Grace Hada October 18, 2025
Stop overcomplicating it-just follow the eccentric plan and you’ll be fine.
alex montana October 18, 2025
Wow!!! This article really hits deep-so much detail, yet I feel something missing?? The pain is real, the science is there-why do we still suffer?!
Wyatt Schwindt October 18, 2025
I see the points you raised and think the practical steps are solid.